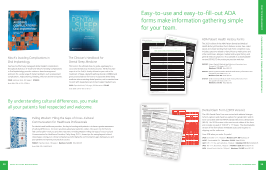
Misch’s Avoiding Complications in Oral Implantology See how to effectively manage all dental implant complications throughout all phases of treatment! Misch’s Avoiding Complications in Oral Implantology provides evidence-based management protocols for a wide range of implant problems such as placement complications, malpositioning, bleeding, infection and nerve injuries. P049 Hardcover book, 891 pages | $198.00 Book ISBN: 978-0-323-37580-1 The Clinician’s Handbook for Dental Sleep Medicine This book is the ultimate how-to guide, a gateway to a successful dental sleep medicine practice. Written by two experts in the field, it clearly delineates your role in the treatment of sleep-related breathing disorders (SRBDs) and gives practical advice for how to incorporate dental sleep medicine into an existing dental practice, not to mention how to work with sleep physicians to best support patient care. P059 Paperback book, 240 pages, 60 illustrations $79.95 Book ISBN: 978-0-86715-813-7 By understanding cultural differences, you make all your patients feel respected and welcome. Pulling Wisdom: Filling the Gaps of Cross-Cultural Communication for Healthcare Professionals For dentists and healthcare providers, the key to bonding with patients is to have a greater awareness of cultural differences. The more you know about your patient’s culture, the easier it is for them to feel comfortable—with you and their treatment. In Pulling Wisdom: Filling the Gaps of Cross-Cultural Communication for Healthcare Providers, Cathy Hung, D.D.S., shares tips for seeing beyond cultural stereotypes, raising your cultural competency and bridging the communication gaps between you and your patients to improve your practice success. P08821 Paperback book, 182 pages | Members $24.95 Retail $36.95 Book ISBN: 978-1642251418 Información del historial médico y dental del pacientePhone:Home A nuestros pacientes: tenga en cuenta que podemos formular preguntas de seguimiento para asegurarnos de que tengamos toda la información que necesitamos a fin de poder tratarlo. INFORMACIÓN DEL PACIENTE Apellido: Nombre: Segundo nombre: Teléfono particular: Teléfono celular: Teléfono laboral: Dirección de correo electrónico: Domicilio postal: Ciudad: Estado: Código postal: Fecha de nacimiento: / / Sexo: Ocupación: Contacto de emergencia: Nombre: Relación: Teléfono: Si está completando el formulario en nombre de otra persona, ¿cuál es su nombre y la relación con esa persona? Nombre: _____________________ Relación: __________________ Si firma este formulario en calidad de representante personal del paciente: Declaro y garantizo que tengo pleno derecho y autoridad legal para consentir la cualquier procedimiento a este paciente. Si por alguna razón ya no tengo tal derecho y autoridad legal, lo notificaré de inmediato por escrito al consultorio.
Medicalrealizaciónlastde HISTORIAL DENTAL Y SÍNTOMAS ¿Cuál es el motivo de la visita de hoy? ¿Actualmente experimenta algún dolor o malestar dental? Sí No Si es así, ¿dónde? ¿Cuándo fue el último examen dental? / / ¿Qué se llevó a cabo en esa cita? ¿Cuándo fue la última vez que le realizaron radiografías dentales? Marque la casilla con una «X» SOLO si se aplica a usted. ¿Le cuesta abrir la boca? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ¿Le duele al masticar, morder o tragar? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ¿Le sangran las encías cuando se cepilla o usa hilo dental? . . . . . . . . . . . . . . . . . . . . . . . . . ¿Se ha sometido alguna vez a tratamientos periodontales (de encías) como destartraje y alisado radicular? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ¿Tiene, o alguna vez ha tenido, llagas o protuberancias en la boca? . . . . . . . . . . . . . . . . . ¿Aprieta o hace rechinar los dientes? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ¿Siente algún chasquido, crujido o dolor en la mandíbula? . . . . . . . . . . . . . . . . . . . . . . . . . . ¿Tiene dolores de oído o de cuello? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ¿El tratamiento dental lo pone nervioso? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ¿Alguna vez ha experimentado alguno de estos trastornos respiratorios relacionados con el sueño? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Respiración por boca Ronquido Dificultad para respirar durante el sueño ¿Alguna vez ha sufrido una lesión grave en la cabeza o la boca? . . . . . . . . . . . . . . . . . . . . Si es así, describa lo ocurrido y cuándo ocurrió: ___________________________________ ____________________________________________________________________________ ¿Ha tenido problemas con el tratamiento dental en el pasado? . . . . . . . . . . . . . . . . . . . . . Si es así, describa lo ocurrido: __________________________________________________ ____________________________________________________________________________n ¿Alguna vez ha tenido una reacción o un problema con la anestesia dental? . . . . . . . . . . Si es así, describa lo ocurrido: __________________________________________________ ____________________________________________________________________________ ¿No le gusta su sonrisa? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Si es así, ¿por qué? Marque donde corresponda: El color de sus dientes La forma de sus dientes La posición de sus dientes Otros. Describa: _________________________________________________________ MEDICACIONES Y OTROS PRODUCTOS/OTRAS SUSTANCIAS Marque las respuestas a las siguientes preguntas con una «X». Sí No ? ¿Toma algún anticoagulante (como warfarina [Coumadin®], rivaroxabán [Xarelto®], dabigatrán [Pradaxa®], clopidogrel [Plavix®], heparina o aspirina)? . . . . . . . . . . . . . . . . . Si es así, ¿qué medicación toma? _______________________________________________________________________________________________________________ ¿Toma alguna medicación para tratar la osteoporosis o la enfermedad de Paget? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Algunos medicamentos que se recetan comúnmente incluyen alendronato (Fosamax®), risedronato (Actonel®), ibandronato (Boniva®), zolendronato (Reclast®) y denosumab (Prolia®). Si es así, ¿qué medicación toma? _______________________________________________________________________________________________________________? ¿Usa, o tiene previsto usar, medicación intravenosa (IV) para tratar el dolor de huesos, la hipercalcemia o las complicaciones óseas derivadas de la enfermedad de Paget, el mieloma múltiple o el cáncer metastásico? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Algunos medicamentos que se recetan comúnmente incluyen denosumab (Xgeva®), pamidronato (Aredia®) o zolendronato (Zometa®). Si es así, ¿qué medicación toma? _________________________________________________ ¿Hace cuántos años que la toma? _______________________________ ¿Recibe terapia de sustitución hormonal?................................................................................................................ ¿Consume algún tipo de tabaco o productos de nicotina (cigarrillo, cigarro, rapé, tabaco para mascar, bidi)? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ¿Utiliza productos de vapeo?............................................................................................................................ ¿Cuántas bebidas alcohólicas consume por semana? __________________ ¿Consume sustancias controladas (drogas), incluida la marihuana, por motivos medicinales o recreativos? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Si es así, ¿qué sustancias?___________________________ Si es así, ¿con qué frecuencia? A diario Varias veces por semana Todas las semanas A veces ¿La sustancia fue recetada por un médico? Sí No Si es así, ¿por qué razones? ____________________________________________________________ ¿Toma algún otro medicamento recetado o de venta libre, vitaminas, hierbas o suplementos? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Si es así, enumérelos aquí e incluya información sobre la cantidad y la frecuencia de uso de cada uno _____________________________________________________ SOLO PARA MUJERES: ¿Toma píldoras anticonceptivas? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ¿Está embarazada? Si es así, incluya la cantidad de semanas: _____________________________ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ¿Está en el periodo de lactancia? Si es así, incluya la cantidad de semanas: ________________ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . © 2021 American Dental Association Formulario S50121 Para volver a pedirlo, llame al 800.947.4746 o visite ADAcatalog.org. Fecha de hoy: ___________________________________ Patient Dental & Medical Health History Information To our patients: know that we may ask follow-up questions to make sure we have all of the information we need in order to treat you. PATIENT INFORMATION Last Name: First Name: Middle Name: Cell Phone: Work Phone: Email Mailing Address: City: State: Zip: Date of Birth: / / Gender: Occupation: Emergency Contact: Name: Relationship: Phone: If you this form for another person, what is your name and to that person? Name: __________________________________ Relationship: _______________ this the I I full legal and authority to to the performance of on this for reason such I the What is the for your visit today? Are any dental pain or discomfort? n Yes n No If yes, where? exam? / / What was done at that appointment?order last had dental x-rays taken? Please mark an in the box if this to you. Is it hard . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . n Does it hurt to chew, bite or . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Do . . . . . . . . . . . . . . . . . . . . . . . . .nn you ever had periodontal (gum) . . . . . . . .n Do you or ever any sores or growths in . . . . . . . . . . .n clench grind your . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . n . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . n . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .nn . . . . . . . . . n n Snoring breathing during sleep Have you ever had a serious injury to your head or mouth? . . . n If ______________________..................... ____________________________________________________________________________ you ever had problems with dental treatment in the If yes, ____________________________________________________________________________....................dentalwith,__________________________________________ you ever had a reaction to, or problem If yes, ____________________________________________________________________________..n.............__________________________________________n unhappy with your smile?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .n If yes, why? all apply: n The color of your teeth n The shape of your teeth n The of your teeth n Other. Please describe: ___________________________________________________ & PRODUCTS/SUBSTANCES the Yes No ? Are you taking any blood thinners Warfarin, rivaroxaban (Xarelto®), dabigatran or . . . . . . . . . . . . . n n n _________________________________________________________________________________________________________position to or Paget’s disease? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . n n n Are you taking, or scheduled to take, an IV to treat bone pain, or . . . . . . . . . . . . . . . . . . . . . . . . . . . . . n n n ___________________________________________ How many years have you been taking it? ________________________... Are you taking ? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . n n n or . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . n n n Do use vaping products . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . n n n How many __________________ you or . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . n n n ________________________________ is your use? n Daily n n Weekly n Occasionally n Yes n No If yes, for what reason(s)? ______________________________________________________________... over-the-counter herbs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . n n n you each Taking birth control pills? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. n n n ___________________ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . n n n Nursing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. n n n 800.947.4746 go ADAcatalog.org. ___________________________________ Child’s Dental & Health History Information To the parents/guardians of the patient: Please know that we may to sure all of we in to treat the patient. PATIENT INFORMATION Name: First Name: Middle / Parent’s/Guardian’s Relationship to Patient: Email Address: Cell Work Phone: State: to Have you adult) or the patient (the child) had? n A than three weeks n A cough that produces blood n Active Tuberculosis Please this form to the right if items. What is the reason for your visit today? How would you describe the patient’s oral health? n Excellent n Good n Fair n Poor discomfort? where? ___________________________________________ If no, when was the patient’s last dental exam? ________________ What was done at that appointment? _________________________________ When the had an to mark Has the patient had any problem with dental treatment in the past? _______________________________________________________________________________.................................................... the had n n n Does the use toothpaste when brushing teeth? n n n How often are the patient’s teeth brushed? ______ time(s) per _______ At what time(s) of day are the teeth brushed? __________ Has the patient ever worn braces or other orthodontic appliances? n n n Has the patient ever had a serious injury to the head, mouth or teeth? n n n If yes, please describe what happened and when it happened: ____________________________________________________________ Does the patient play any contact sports or participate in active recreational activities? n n n If yes, please describe those activities here: ___________________________________________________________________________ Is your home water supply fluoridated? n n n What is the patient’s primary source of drinking water? n Tap n Bottled n Filtered n Well Does the patient take fluoride supplements? n n n Does/did the patient use a pacifier or suck his/her thumb or fingers? n n n At what age did the patient stop breastfeeding? __________ At what age did the patient stop bottle feeding? __________ Has the patient ever experienced any sleep-related breathing disorders? n Mouth breathing n Snoring n Trouble breathing during sleep © 2021 American Dental Association Form S70721 To reorder call 800.947.4746 or go to ADAcatalog.org. ___________________________________ Dental Claim Form (2019 Version) The ADA Dental Claim Form was revised with editorial changes to form captions and check box options for gender (M, F and U) to be consistent with the HIPAA standard electronic dental claim (837D). The 2019 version is the most recent edition of the form and includes one pad of 100 8.5" x 11" sheets. The downloadable version of the form allows immediate access and requires no shipping not for online use. Save 20% when you order 5+ packs! J430 (shown) 8½” x 11”, 100/pad | Members $14.95 Retail $22.95 J430T Downloadable PDF | Members $19.95 Retail $29.95 J431 8.5” x 11”, Two-part carbonless, 100/pack | Members $19.95 Retail $29.95 J432 8.5” x 11”, Bond Stock, 250/pack | Members $29.95 Retail $44.95 J434 (shown) Bond in Red Ink, 100/pad | Members $14.95 Retail $22.95 ADA Patient Health History Forms The 2021 edition of the ADA Patient Dental and Medical Health History Information Form features a clear, two-sided layout and simple wording that make form completion easy. Includes questions related to dental history, medications and other substances, allergies, medical and surgical history and general medical symptoms. Also available as a downloadable version (S50021T) for posting on practice web sites. S50021 Patient Dental & Medical Health History Information Form One pad of 100 sheets, 8.5” x 11” Members $19.95 Retail $29.95 S50121 Spanish | Patient Dental & Medical Health History Information Form One pad of 100 sheets, 8.5” x 11” Members $19.95 Retail $29.95 S70721 Child’s Dental and Medical Health History Information Form One pad of 100 sheets, 8.5” x 11” Members $19.95 Retail $29.95 Easy-to-use and easy-to-fill-out ADA forms make information gathering simple for your team. and J434 shown RECORD OF SERVICES PROVIDED 24. Procedure Date (MM/DD/CCYY) 25. Area of Oral Cavity 26. Tooth System 27. Tooth Number(s) or Letter(s) 28. Tooth Surface 29. Procedure Code 29a. Diag. Pointer 29b. Qty. 30. Description 31. Fee 1 2 3 4 5 6 7 8 9 10 33. Missing Teeth Information (Place an “X” on each missing tooth.) 34. Diagnosis Code List Qualifier ( ICD-10 = AB ) 31a. Other Fee(s) 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 34a. Diagnosis Code(s) A _________________ C _________________ 32 31 30 29 28 27 26 25 24 23 22 21 20 19 18 17 (Primary diagnosis in “A”) B _________________ D _________________ 32. Total Fee 35. Remarks AUTHORIZATIONS ANCILLARY CLAIM/TREATMENT INFORMATION 36. I have been informed of the treatment plan and associated fees. I agree to be responsible for all charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or the treating dentist or dental practice has a contractual agreement with my plan prohibiting all or a portion of such charges. To the extent permitted by law, I consent to your use and disclosure of my protected health information to carry out payment activities in connection with this claim. X _____________________________________________________________________________ Patient/Guardian Signature Date 38. Place of Treatment n (e.g. 11=office 22=O/P Hospital) (Use “Place of Service Codes for Professional Claims”) 39. Enclosures (Y or N) 40. Is Treatment for Orthodontics? No (Skip 41-42) Yes (Complete 41-42) 41. Date Appliance Placed (MM/DD/CCYY) 42. Months of Treatment 43. Replacement of Prosthesis No Yes (Complete 44) 44. Date of Prior Placement (MM/DD/CCYY) 37. I hereby authorize and direct payment of the dental benefits otherwise payable to me, directly to the below named dentist or dental entity. X _____________________________________________________________________________ Subscriber Signature Date 45. Treatment Resulting from Occupational illness/injury Auto accident Other accident 46. Date of Accident (MM/DD/CCYY) 47. Auto Accident State BILLING DENTIST OR DENTAL ENTITY (Leave blank if dentist or dental entity is not submitting claim on behalf of the patient or insured/subscriber.) TREATING DENTIST AND TREATMENT LOCATION INFORMATION 53. I hereby certify that the procedures as indicated by date are in progress (for procedures that require multiple visits) or have been completed. X________________________________________________________________________________ Signed (Treating Dentist) Date 48. Name, Address, City, State, Zip Code 54.
J430 NPI 55. License Number 56. Address, City, State, Zip Code 56a. Provider Specialty Code 49. NPI 50. License Number 51. SSN or TIN 52. Phone Number ( ) - 52a. Additional Provider ID 57. Phone Number ( ) - 58. Additional Provider ID HEADER INFORMATION 1. Type of Transaction (Mark all applicable boxes) Statement of Actual Services Request for Predetermination/Preauthorization EPSDT / Title XIX 2. Predetermination/Preauthorization Number DENTAL BENEFIT PLAN INFORMATION 3. Company/Plan Name, Address, City, State, Zip Code OTHER COVERAGE (Mark applicable box and complete items 5-11. If none, leave blank.) 4. Dental? Medical? (If both, complete 5-11 for dental only.) 5. Name of Policyholder/Subscriber in #4 (Last, First, Middle Initial, Suffix) 6. Date of Birth (MM/DD/CCYY) 7. Gender M F U 8.Policyholder/Subscriber ID (Assigned by Plan) 9. Plan/Group Number 10. Patient’s Relationship to Person named in #5 Self Spouse Dependent Other 11. Other Insurance Company/Dental Benefit Plan Name, Address, City, State, Zip Code POLICYHOLDER/SUBSCRIBER INFORMATION (Assigned by Plan Named in #3) 12. Policyholder/Subscriber Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code 13. Date of Birth (MM/DD/CCYY) 14. Gender M F U 15.Policyholder/Subscriber ID (Assigned by Plan) 16. Plan/Group Number 17. Employer Name PATIENT INFORMATION 18. Relationship to Policyholder/Subscriber in #12 Above Self Spouse Dependent Child Other 19. Reserved For Future Use 20. Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code 21. Date of Birth (MM/DD/CCYY) 22. Gender M F U 23. Patient ID/Account # (Assigned by Dentist) ©2019 American Dental Association J434 (Same as ADA Dental Claim Form – J430, J431, J432, J433, J430D) Dental Claim Form To reorder call 800.947.4746 or go online at ADAcatalog.org ORDER BY PHONE: 800.947.4746 38 39 ORDER ONLINE: ADASTORE.ORG fold fold PRACTICE MANAGEMENT CLINICAL RESOURCES | FORMS AND OFFICE ESSENTIALS fold fold
Purchased by , From: ADA Ebooks (ebooks.ada.org)